

Muscles degenerate and are affected by ALS all over the body, including core life sustaining systems like breathing and swallowing. For a majority of ALS people, the first symptoms start in the limbs and gradually over time move toward the core of the body and eventually end up impacting muscles in the chest, neck and face. There are some patients that ALS affects their neck and chest muscles as the first symptoms, this is called bulbar symptom onset. In all cases though, the ability to chew and swallow food, as well as manage saliva become difficult as the muscles weaken. Because of this muscle weakness a person cannot eat normally or it becomes difficult to the point that nutrition and maintaining weight is a primary concern. This is where the feeding tube comes into play and is a direct method of introducing both food and liquids into the stomach.
As the muscles in the diaphragm and chest area begin to be impacted, the ability to draw and exhale breath gets diminished. For example, at the beginning of 2023 I would consider my breathing capacity to be normal but towards the middle of 2024 my overall lung capacity had decreased to 71%. Every quarter I go to what’s called a clinic day where we measure and quantify progression including lung capacity and at my last measurement my lung capacity has decreased to 61%. This is significant because any surgeries where anesthesia might be required are generally not recommended for ALS patients if their lung capacity is less than 50%. So as a follow up to my last clinic day it was recommended that I get the feeding tube surgery sooner rather than later to ensure that it could be done successfully with lung capacity above 50%.
I took a few days to think over the procedure and process, even though I knew my eventual answer would be yes, because it represents a significant milestone in my progression. It is very difficult to think about not being able to eat, drink and eventually speak and the feeding tube is a daily reminder of that eventuality. Right now, I am just happy that it is not necessary and hopefully won’t be for a significant amount of time. We scheduled the surgery for early December however, some other medical issues prevented me from getting it done in that time frame so we rescheduled to after the holiday season. It was a little surreal for me to think about my one year anniversary of being diagnosed on January 8th and then getting a feeding tube installed just a few days after that anniversary.
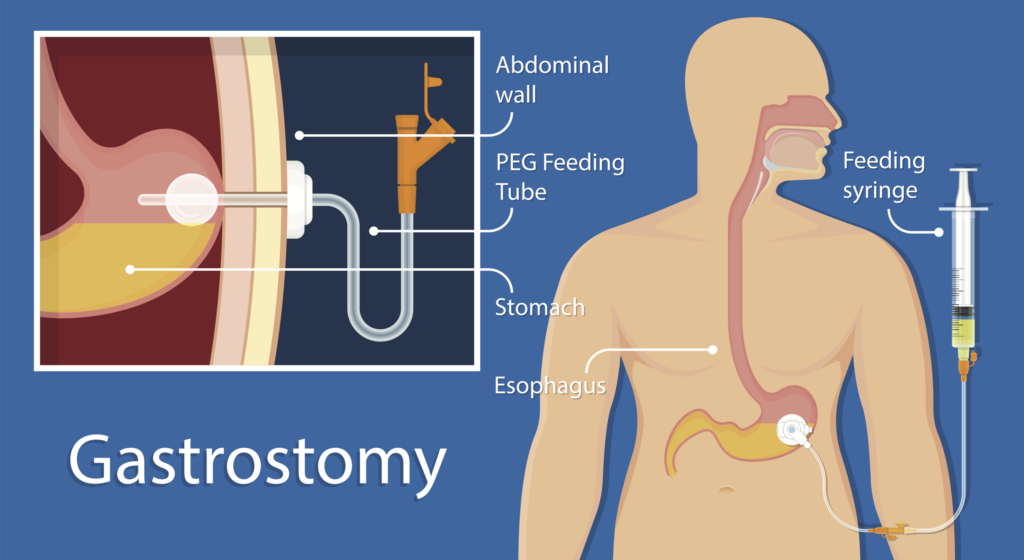
Image Source: https://www.doctorlansford.com/lc-g-tube-placement
In preparation for the surgery I had to fast 12 hours before showing up to the appointment which included no drinking as well so I was already starting to get hangry. At about 18 hours before the surgery I had to drink a barium sulfate contrast liquid so that they could use that to X-ray my stomach and bowel areas during the procedure. Whoever invented or came up with this drink should have to drink it every day for the rest of their life! This semi liquid was the consistency of Elmer’s glue and tasted horrible. I could only get it down using rapid draws with a fat straw so that I didn’t have to taste as much of it. The taste was so bad that I’m pretty sure they made it gross on purpose to prevent people from drinking it voluntarily.
On the morning of the procedure we made our way to the Seattle VA hospital and checked in at the same day surgical unit. They got me prepped and ready for surgery fairly quickly and I was in the operating room around 11:00 AM. Because ALS has significant breathing complications possible during surgeries they usually do not fully sedate the patient. In my case, they only gave me some nausea medicine and fentanyl for pain. Fentanyl is a magic drug that I have had only twice before and it’s the only two times in over a decade that I was fully pain free for the 30 minutes or so that the drug lasts. So now we are prepped and ready for the procedure to start and I’m very awake and nervous.
As it was explained to me we basically were going to pump my stomach full of air and the doctor was going to make a small incision and insert the feeding tube along with a balloon system that seals it from the inside. To pump the air into the stomach you have to have a tube inserted through your nostril that goes down the back of your throat and all the way to your stomach. The first step was a lidocaine Jelly that is injected into the nasal cavity through a syringe. This felt pretty gross and wasn’t too bad because it instantly started to desensitize the area. The next step was probably the worst part of the procedure for me, and that was the insertion of about 30 inches of tube that was fed through the nostril down the throat and into the stomach. The medical technician performing this procedure was a rather large and muscular Nigerian man who said take a deep breath and let’s get the hard part over with. The first try didn’t go so good because I think the tubing tried to go down my esophagus instead of to my stomach. This caused me to wretch, cough and cry for about 10 minutes after we aborted that attempt. So now we had to start over again with the lidocaine Jelly with round two. This time the insertion process went much better and one of the things they tell you to do is try and swallow to get the tubing to go down easier. Thinking back on that specific moment all I can remember is a large man telling me to swallow swallow swallow and my mind playing funny tricks said “did I go to prison and not remember?!” We finally got the tube in place and a little bit more fentanyl on board and we were ready to start the actual procedure.
To start off the procedure they begin pumping air into your stomach and this can cause nausea, and it did for me. They gave me a stronger anti nausea medication that acted very quickly and made the rest of the procedure bearable. From the start of the procedure to fully completed took about 35 minutes. The doctor had an up-and-coming trainee (fellowship) that she was teaching so it took a few minutes longer than typical. Once all the scrubbing and prep work were completed, they gave me four shots of lidocaine in the local area and performed the incision and insertion process. During this 30-minute window I was using every mental and breathing technique I have ever learned to maintain calm as well as manage the feeling of nausea. I hate having congestion in my nose as well as the feeling of something dripping down the back of my throat, so this was particularly challenging. It seemed like forever, but the procedure was finally over and the last uncomfortable process was removing the nasal tube which was done in one quick draw motion. The lidocaine effects numbing the back of my throat and nostril were very much appreciated at that moment.
After the procedure I got to go to the recovery area and then eventually to a regular hospital room for observation until noon the next day. The feeding tube was attached to a discharge collection bag that filled up gradually as liquids from my stomach were expelled. This was a little challenging when getting up to go to the bathroom having a bag on one side of you and an IV on the other side. I still was not able to eat until breakfast the following day and I was extremely hungry and feeling dehydrated at that point. The only liquids I had consumed was sucking on a spongy swab to keep my mouth and lips moist. One other thing that was making me uncomfortable was the lack of medications that I was allowed to consume during that 18 hour window. I typically take pain medication every six hours so the other parts of me that are broke were starting to Get more intense. Finally for breakfast around 9:00 AM I got my first pain medications and a little bit of food water and orange juice.
So overall I’m glad I got the procedure done although it does add a new level of complexity to managing ALS for me. My wife will now have to flush the feeding tube four to six times a day with clean water to make sure it stays open. At the hospital I got a little bit of training on maintenance and use and my wife got training from the nurse who showed her how to flush and went over general precautions and possible complications.

